
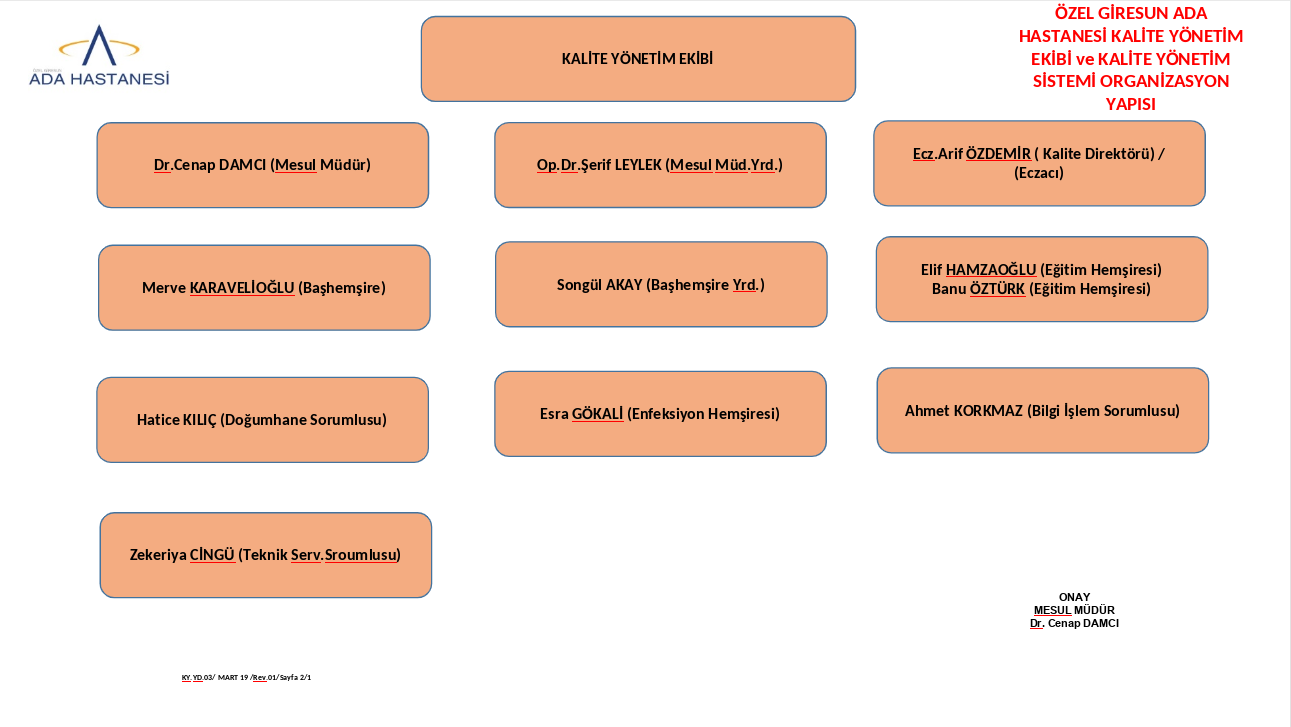
Ada Hospital Quality Management Directorate
Our hospital quality management unit quality director Ecz. Arif ÖZDEMİR and the quality management team coordinate the work carried out within the framework of SKS.
OUR QUALITY UNIT
- Provides follow-up of the studies for corporate goals and objectives.
- Manages self-assessments.
- Manages the processes related to the security reporting system.
- Manages the processes related to risk management.
- Manages studies to measure patient and employee experiences (such as survey applications, evaluation of survey results, improvement studies for survey results, patient and employee feedback).
- Provides management of documents within the framework of SKS.
- Manages processes for quality indicators.
- Participates as a member of the committees determined within the framework of the SCS.
ACTIVITIES
Corporate Goals and Objectives:
The process of realizing the goals and objectives determined annually is monitored every 6 months and the results are evaluated at the end of the year. The results of the analysis of the goals and objectives for their realization are reported to the employees of the institution.
Self-Assessment Activities:
In our hospital, a self-evaluation plan including all SKS standards is prepared once a year with the quality management unit and self-evaluation team. In the plan, the team that will make the self-evaluation and their dates are determined and announced to all departments.
Corrective preventive action is initiated for the nonconformities identified as a result of the self-evaluation and the process of eliminating the nonconformity is followed by the quality unit. The result of the DÖF is evaluated according to the specified deadline. If the problem is solved, it is closed, if not, the root cause analysis is performed and the date of the DÖF is extended.
The results of the self-evaluation are reported to the management.
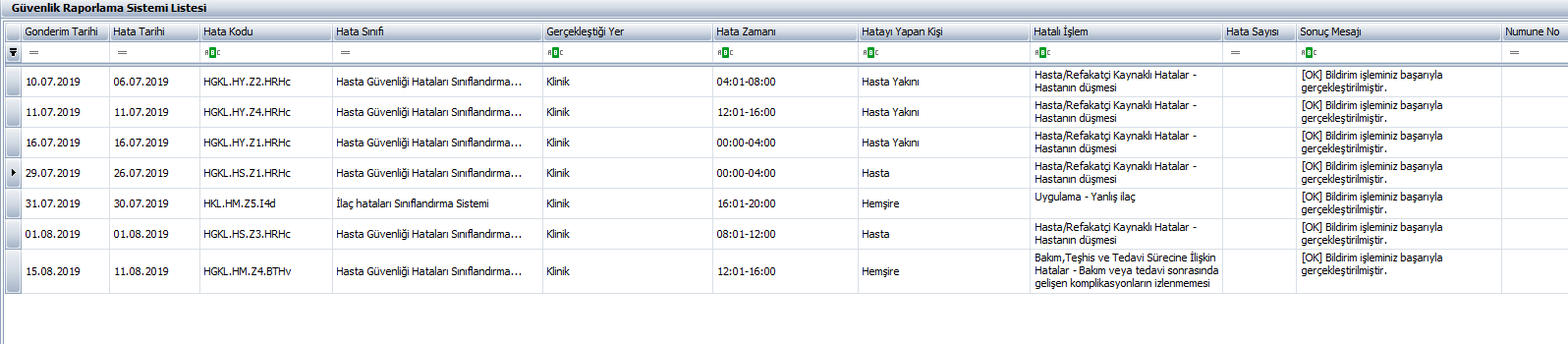
Security Reporting System:
In our hospital; It is used to ensure that unwanted events that may threaten the safety of patients and employees, that do not occur at the last moment (near the moment) or that occur when they are about to occur are notified, to monitor these events, and to ensure that the necessary measures are taken for the events as a result of the notifications. The main objectives are to ensure Patient Safety and to provide a Healthy Working Life environment.
Risk Management:
Within the scope of patient, patient relative, visitor, employee and facility and environmental safety, we aim to ensure patient safety and to realize healthy working life effectively and effectively in order to prevent or minimize the risks related to our hospital and all services offered in our hospital.
With the evaluation of the hospital manager, occupational health and safety unit responsible and occupational health and safety experts, risks are determined and a follow-up process is carried out in accordance with the planning.
Measuring Patient and Employee Experiences:
Patient experience surveys are conducted every month as emergency, outpatient and inpatient. A survey is conducted once a year for employees: All data are analyzed by the Quality Management Unit and these data are brought up in the relevant committee and team meetings. The results of the annual survey are reported to the entire hospital.
In addition to the survey application, notifications made to the wishes, suggestions and complaints boxes within the hospital, applications made to the patient rights unit, suggestions and complaints of patients and employees made through the hospital web page and hastahaklari.saglik.gov.tr address are evaluated monthly.
Management of Documents within the Framework of SKS:
Our hospital has accepted the SKS Document Management System Guide published by the Department of Quality and Accreditation in Health of the General Directorate of Health Services of the Ministry of Health as an outsource of the Document Management System procedure. And all the documents used in our hospital are prepared in the light of this guide. The Quality Management Unit is responsible for the control of the documents. All employees can access the documents through the intranet system of our hospital with a common network.
Documents Used in Our Hospital:
It consists of procedures, instructions, guides, forms, plans, consent documents, lists, auxiliary documents.
All other documents hanging in the hospital are hung within a certain control and order.
Quality Indicators:
Department-based and clinic-based indicators are collected through data collection according to the Ministry of Health indicator management guide and SKS standards and transmitted to the relevant institution. The indicators to be notified in the indicator notification area on the Corporate Quality System web page are entered into the relevant fields with the data collected in 3-month periods. The whole process is coordinated by the Quality Unit and the indicator responsibles. The result value is compared with the target value to analyze and interpret the results obtained. If the results of the analysis show a negative deviation from the target value, root cause analysis is performed to reveal the conditions that cause the deviation. Whether the result is positive or negative, the critical points in achieving this result are evaluated.
Committees Determined within the Framework of the SCS:
The committees in our hospital in accordance with SKS standards are as follows:
- Patient Safety Committee
- Employee Health and Safety Committee
- Education Committee
- Facility Safety Committee
- Infection Control Committee
Patient Safety Committee: It operates to determine possible risks in a way that will ensure the effectiveness, continuity and systematicity of the studies carried out in the hospital, to determine the appropriate methods and techniques to eliminate these risks, and to ensure the sustainability of safe service delivery and safe working environment with in-service trainings. The Committee meets at regular intervals at least four times a year and when necessary.
Quality Management Team: The team organizes meetings with department quality officers, hospital management and quality management unit and evaluates quality activities. The team evaluates quality activities such as corporate goals and objectives, indicator data, corrective preventive actions, follow-up of self-assessment nonconformities.